Conference Lectures
Lung Protective Ventilation: ICU practice in operation theatre
Dr S Bala Bhaskar
Introduction: Ventilation is the sine-qua-non of major general anaesthesia procedures and is associated with numerous effects on physiology. Pulmonary complications have been recognized from the earlier days of general anaesthesia. The term ‘‘ether pneumonia’’ was used in 1920, demonstrating the long-standing association between anaesthesia, surgical procedures and pulmonary complications (1,2). In average adult patients without any significant respiratory and cardiac comorbidities, volume controlled ventilation is the standard practice under muscle paralysis. Millions of patients have been ventilated with high tidal volume (TV) as a traditional setting including those with lung injury and in thoracic and cardiac surgery scenarios, presumably to prevent atelectasis.(3) Anaesthesiologists in addition used higher FiO2 and peak inspiratory pressures to improve oxygenation during ventilation for many years in non OLV and non-cardiac settings as well. However, the persistence of pulmonary complications in the postoperative period prompted investigators to apply the experience gained in ventilation of patients in intensive care units (ICUs), the ‘lung protection ventilation’ strategies to intraoperative period as well and assess the benefits if any.
The pulmonary dysfunction:
Post-operative pulmonary dysfunction can manifest as hypoxia, laryngospasm, bronchospasm, aspiration pneumonitis, atelectasis, respiratory infections, respiratory failure and acute respiratory distress syndrome.(1,4,5) (ref A and 1,2) The incidence of post-operative pulmonary complications (PPCs) after non-cardiac surgery is comparable with that of cardiac complications (2.7% vs 2.5%, respectively) (6) and can delay hospital discharge and increase in morbidity and mortality.(1,4,5) (ref A and 1,2). National Surgical Quality Improvement Project (NSQIP) database found that independent of preoperative risk, PPCs were associated with a significant increase in mortality from 2% to 22% . (1,7) The impact of PPCs on mortality is similar in other studies; one of which showed an overall incidence of PPC of 5% and a 30-day mortality of 19.5% in patients with a PPC versus only 0.5% in patients without a PPC .(1,4,5)(ref A and 1,2).
The injury to lungs: the concepts and causes
The mechanical ventilation administered as during ICU care and during prolonged general anaesthesia is associated with lung injuries if the mechanics of the lung are disturbed due to variations in the ventilatory parameters related to volumes and pressures for an individual patient. Excessive tidal volume (volutrauma),elevated airway pressures (barotrauma), injury related to repeated collapse and opening of alveoli (atelectrauma) and release of inflammatory mediators (biotrauma) lead to ventilator-induced lung injury (VILI) and acute respiratory distress syndrome (ARDS).(1,8) The phenomenon of VILI is well recognized. VILI can exacerbate existing lung injury or sensitize the lung to further injury (the so-called two-hit model, which is significant with large transfusions, CPB, and associated lung ischaemia–reperfusion injury).
Volutrauma may occur from the application of large tidal volumes with alveolar overdistension, epithelial injury, and resultant local and systemic inflammation. Volutrauma initially results in loss of active functioning areas but may precipitate a self-perpetuating phenomenon with the remaining functional alveoli bearing the brunt of accommodating increased local tidal volumes due to reduced overall lung volume.
Barotrauma is less common and may manifest as pneumothorax or pneumomediastinum. Thus, the main aim to avoid injury would be to avoid large tidal volumes and high plateau airway pressures.
The benefit of applying positive end-expiratory pressure (PEEP) in preventing alveolar collapse and resultant atelectrauma is well known. The optimal PEEP is however subject to discussion; it is said that higher PEEP levels are beneficial in those with severe ARDS, but harmful in patients with milder forms of ARDS(9) Hyperoxia and risk of oxygen toxicity are known entities with potential for lung injury, depending on duration of exposure. Higher FiO2 (>0.6) is used during preoxygenation but sustained hyperoxia is not common.(10)The effects include absorption atelectasis, decreased mucociliary clearance, decreased surfactant production, and free radical formation. It is unclear how, or if, these observations translate into clinically relevant acute PPCs. Evidences have shown mixed results, some showing adverse effects and some no changes.(11,12)Patients on bleomycin are probably under risk of hyperoxia induced lung toxicity and again there are contradictory evidences.
Studies in intensive care units (ICU) and operation theatres (OT) have showed significant lung damage including acute lung injury, with high TV ventilation. It is reported that 24% of the patients with normal lungs ventilated in an ICU setting for 2 days or longer developed acute lung injury (ALI) or acute respiratory distress syndrome (ARDS).(13)In another study, it was reported that TV >700 ml and peak airway pressures (PAP) >30 cm H2O were independently associated with the development of ARDS.(14)
The adverse effects of large TVs: A study in patients undergoing oesophageal surgery compared the use of tidal volumes of 9 ml/ kg without positive end expiratory pressure (PEEP) during two and one lung ventilation (OLV) vs 9 ml/kg during two-lung ventilation and 5 ml/ kg during OLV with PEEP of 5 cm H2O. They found significantly lower serum makers of inflammation [IL-b, IL-6, and IL-8] in the lower TV plus PEEP group. The study demonstrated better oxygenation in the lower TV group during and immediately after OLV, with earlier extubation (postoperative mechanical ventilation duration, 115 vs 171 min).(15) Larger TV have been found to be associated with greater release of pro inflammatory mediators and procoagulant changes in bronchial lavage fluid.(16,17)A study in patients without lung injury undergoing major surgery (> 5 h duration), mechanical ventilation (MV) with higher TV of 12 ml/kg ideal body weight without PEEP or lower TV of 6 ml/kg with 10 cm H2O PEEP were compared. After induction of anaesthesia and 5 h thereafter, bronchoalveolar lavage fluid and/or blood was investigated for polymorphonuclear (PMN) cell influx, changes in levels of inflammatory markers, and nucleosomes. They concluded that the use of lower tidal volumes with PEEP may limit pulmonary inflammation in mechanically ventilated patients without pre-existing lung injury.(18)
Strategies to prevent PPCs: The PPCs can be reduced or prevented by certain ventilatory and non ventilatory measures. Indirect or non ventilatory factors which contribute to the development of pulmonary complications intra operatively and post operatively have to be attended to simultaneously with application of ventilatory strategies.
The Lung Protective Ventilation Strategies:
Benefits of use of lung protective ventilation (LPV) strategies specifically for the treatment of ARDS has been supported by good evidences and recently, LPV strategies (table 1) have been found to be useful in patients without ARDS.
Strategy |
Rationale |
Lung Protective Ventilation |
For ARDS,significant mortality benefit |
Positive End Expiratory Pressure |
Improves oxygenation |
Recruitment Manouevres |
Improves oxygention |
Table 1. Mechanical ventilation strategies to prevent PPCs (1)
During mechanical ventilation, the main considerations are protection against over-distension of alveoli (volutrauma) in addition to the repeated opening and closing of lung segments at low lung volumes (atelectrauma), the first effect being overcome by limiting tidal volume (and consequently also plateau pressures) and second, by applying PEEP to prevent atelectasis.
The Low TV: The benefits of application of LPV during the relatively brief duration of MV in operation theatres were not optimistically looked at initially as compared to proven benefits with longer duration of ventilation in ICUs.
The low TV benefit was well demonstrated during the ARDS net trial (2000); significant mortality benefit (31% vs 39.8%) and more ventilator-free days were observed with the low tidal volume strategy (6 mL/kg ideal body weight [IBW]) versus ‘‘traditional’’ TV (12 mL/kg IBW). (19)It is recommended to base TV settings on IBW rather than actual body weight and the gender for LPV as lung size is estimated from gender and height.
Atleast 40 studies were conducted on non ARDS groups of patients after the year 2000, assessing the potential benefits of LPV strategies. A meta-analysis (2012)(20) compared the results in patients in the operating room and in the intensive care unit (ICU).Significant reduction in the development of ARDS with LPV strategies was demonstrated. There was also a decrease in pulmonary infections and reduced length of stay in hospital with LPV.
Hemmes SN and others in a meta-analysis demonstrated the benefits of LPV in patients receiving MV for short duration during surgeries (lower risk of developing ARDS or pulmonary infection.(21)Higher levels of PEEP were associated with lower rates of ARDS and pulmonary infections.(22)
In another meta-analysis of studies using low TV as part of lung protective strategy in patients without ARDS, it was found that the clinical outcomes were better with low TV. The limitations were that the mechanically ventilated patients in both intensive care units and operating rooms were subjects and the duration of mechanical ventilation varied. In a study published recently (2013) of patients undergoing open abdominal procedures, a LPV strategy (tidal volumes of 7 mL/kg with 10 cm H2O PEEP) was compared with traditional ventilation (9 mL/kg tidal volume without PEEP); there was decrease in pulmonary infections, improved postoperative oxygenation, and decrease in postoperative atelectasis. (23) Use of low tidal volumes with PEEP was better than use of low TV without PEEP (6 mL/kg tidal volumes and 12 cm H2O of PEEP with 6 mL/kg tidal volumes and no PEEP) in a group of elderly patients during intraoperative MV in regard to respiratory mechanics and oxygenation intraoperatively but not postoperatively but power of study was low.
Role of PEEP: Studies correlating use of PEEP during GA and mortality are limited. A Cochrane review showed an association between intraoperative PEEP and oxygenation (increased PaO2/FiO2 on postoperative day 1 and decreased postoperative atelectasis(24)but no adequately powered mortality data is available.(24)
Recruitment manoeuvres aim to recruit collapsed alveoli to improve oxygenation and prevent low-volume lung injury. In a study during abdominal laparoscopic procedures, application of recruitment manoeuvres resulted in a positive effect on oxygenation and compliance. PEEP alone and PEEP plus recruitment manoeuvres were compared; improved intraoperative oxygenation and compliance with PEEP plus recruitment manoeuvres were demonstrated.(25) No postoperative pulmonary outcomes were noted and outcomes were also not studied in the trial.
Hypercapnoea: Permissive hypercapnoea, or hypercapnoeic acidosis (HCA), is an accepted consequence of lung protective ventilation in patients with ALI/ARDS. Although conventional wisdom holds that HCA is a consequence of relative hypoventilation, HCA per se has protective effects on the pathogenesis of ALI. HCA is protective in many models of ALI. Beneficial effects include attenuation of lung PMN recruitment, pulmonary and systemic cytokine concentrations, cell apoptosis, and free radical injury. In several animal models, HCA attenuated free radical-mediated lung injury by inhibiting endogenous xanthine oxidase and attenuated lung injury in both early and prolonged sepsis. Acidosis and hypercapnoea might exert distinct biological effects, but this remains to be elucidated.
The problems with low tidal volumes:
At the other end, questions have been raised on the benefits in patients with healthy lungs when the so called lung protective settings are used and that they could even be harmful. Study using a murine ‘one hit’ ventilator-induced lung injury (VILI) model showed that even the least injurious volume settings induced biochemical and histological changes consistent with lung injury.(26) Work with rodents undergoing mechanical ventilation showed significant gene expression (including genes involved in immunity and inflammation such as IL-1b and IL-6) after only 90 min of protective ventilation in the absence of a primary pulmonary insult.(27)
Thus, it is also important to know that there is possibility that non-physiological ventilation (ventilation with larger TV) in healthy lungs induces ALI and protective lung ventilation in non-injured lungs and in the absence of a primary pulmonary insult may initiate subclinical VILI, as evidenced by gene expression and inflammatory markers, and possibly sensitize the lung to a ‘second hit’.
Measures to reduce PPCs by non-ventilation strategies:
There are many risk factors and causes with basically non respiratory origin for post-operative pulmonary complications and these have to be attended to while attempting to reduce the PPCs.(1,28)
Non ventilatory risk factors for perioperative pulmonary complications:
The risks can be related to the patient or to the procedure. The management of the ventilation is influenced by the presence of risk factors in the preoperative period. Advanced age, functional limitation, ASA II and more, congestive heart failure, COPD, etc are some of the major factors contributing to risk of pulmonary complications. Similarly, certain procedures are more likely to cause PPCs such as major intravascular, intrathoracic, intracranial procedures, prolonged surgeries, etc (table 2).(1,29)
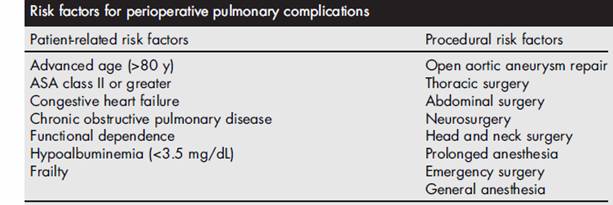
Table 2. Risk Factors for perioperative pulmonary complications
Preoperative functional status can also affect incidence of PPCs as quantified by a frailty index (such as the Canadian Study of Health and Aging Clinical Frailty Scale).(1,30)
Obstructive sleep apnoea (OSA) is an independent risk factor for PPCs including aspiration, pulmonary embolism, and requirement for mechanical ventilation.(31)It is associated with increased risk of hypoxic and hypercapnoeic responses to anaesthetic agents, sedatives and analgesics, and microaspiration.
Non ventilatory / indirect causes of post-operative pulmonary complications (table(3)
Prevention of gastric-to-pulmonary aspiration:
Among the well-known factors causing lung injury in perioperative period is the aspiration of regurgitated contents. Regurgitation and aspiration due to sedation and loss of protective reflexes due to drugs, disease and surgery can cause various degrees of pulmonary dysfunction. The use of the head-of-bed elevation has been shown to reduce risk of aspiration in ICU settings (32) and the same can also
Regurgitation aspiration
Blood transfusion related
Direct Lung Injury
Smoking
General anaesthesia
Neuromuscular block and reversal
Atlectasis
Sedation and Opioids
Intravenous Overhydration
Table 3. Causes of postoperative respiratory impairment/ injury (1)
be useful in prolonged surgeries. The application of cricoid pressure is a standard practice along with rapid sequence induction and intubation but there are no clear cut evidences to support the practice.(33,34)Micro aspiration is likely to be associated with ARDS and VAP. Preventive measures used against macroaspiration are also applicable against micro aspiration.(35,36)
Transfusion related acute lung injury:
Blood transfusion is associated with risk of lung injury: transfusion-related acute lung injury (TRALI) and transfusion-associated circulatory overload (TACO). TACO might be related to volume overload and elevated left atrial filling pressures, resulting in hydrostatic pulmonary oedema and associated hypoxemia. Advanced age, ventricular dysfunction, and total volume of blood product transfused are determinants of TACO.(37)
TRALI results in injury to pulmonary endothelium due to activation of neutrophils by donor antibodies with development of non-hydrostatic pulmonary oedema and hypoxemia.(38)
TRALI is more common with transfusion of plasma-rich blood products (such as fresh frozen plasma or apheresis platelets).(39) TRALI is associated with other risk factors such as liver transplantation surgery, chronic alcohol abuse, shock, use of higher peak airway pressures during mechanical ventilation, smoking, and positive fluid balance.(40)
Preventing transfusion-related acute lung injury: The experience gained on transfusion related lung injury in ICUs can be applied in operation theatres. Unnecessary administration of blood products is advised to be avoided but when it is mandatory, alternative strategies for TRALI prevention have to be used. Among the most effective methods, one is the transition to male-only plasma donation which is associated with a significant reduction in TRALI incidence when compared with a historical cohort (OR 0.21).(41) It is suggested that prolonged duration of red blood cell (RBC) storage may precipitate risk of adverse respiratory outcomes but evidences are inconclusive.(42)
Anaesthetic and analgesic techniques:
Inhalational versus intravenous anaesthesia: No significant differences have been found with respect to PPCs between inhalational or total intravenous anaesthesia (TIVA). Sevoflurane as inhalational anaesthetic compared to TIVA (with propofol and remifentanil) during oesophagectomy did not demonstrate a significant difference in PPCs.(43)
Effects of sedation and lung functions: Opioid analgesics, benzodiazepines and many anaesthetic agents inhibit the central respiratory drive and the protective airway reflexes, and thus increase the risk for PPCs. Some patients may develop delirium after prolonged sedation affecting extubation. Deep sedation also causes delay in extubation and increased mortality. Dexmedetomidine as an alpha 2 agonist has the potential to reduce the risk of PPCs avoiding/reducing opioid induced adverse effects.(44)
Effects of anaesthetic agents and muscle relaxants on diaphragmatic function and chest wall mechanics: These are commonly mentioned causes related to PPCs. Residual neuromuscular blockade has to be assessed in the background of residual sedation and anaesthetic effects. Regional anaesthesia and analgesia reduce such the incidence of pulmonary complications. Residual neuromuscular blockade is a likely contributor to PPCs. Significant residual NM blockade can precipitate acute respiratory failure postoperatively as reported in large case-control study.(45,46) It has been found in a prospective study that forced vital capacity (FVC)was reduced to 62% of baseline despite adequate (train-of-four [TOF] ³ 0.9) reversal and even greater reduction (FVC= 49% baseline) in the presence of residual (TOF <0.9) neuromuscular blockade.
Effect of residual neuromuscular blockade after GA: The initial target TOF ratio of 0.7 as an end point of adequate reversal of non-depolarising blockade is revised to atleast 0.9. TOF of 0.7 correlates with normal tidal volumes, sustained eye opening, tongue protrusion, and handgrip and a ratio of 0.7 to 0.9 correlates with sustained head lift and sustained leg lift, but cannot guarantee adequate recovery and hence the risk of PPCs persists.(47) Lung mechanics, including a low FVC is common and residual Oropharyngeal muscle weakness can lead to upper airway obstruction, hypoxia and aspiration.It is advised to monitor the blockade recovery and avoid long acting relaxants.
Postoperative analgesia: Type of analgesia and quality of analgesia will influence the incidence of PPCs. The analgesic technique/drug should not induce deep sedation, inhibit ability to take deep breaths and produce effective cough. Epidural analgesia improves vital capacity by 18% and functional residual capacity by 5.8% following major abdominal surgery.(48) The reduction in PPCs is also related to reduction in consumption of opioids after epidural analgesia and have been reported with wide variety of surgeries including cardiac. thoracic, major abdominal surgeries and fast track procedures.(49,50)
Effect of combining regional analgesia and general anaesthesia (51,52,53): The evidences have been conflicting with some studies demonstrating decrease in PPCs and others showing no significant benefits. Single-shot femoral nerve block to GA for total knee arthroplasty increased oxygen saturation in the immediate postoperative period.
Smoking and smoking cessation: Smoking cessation at any point preoperatively is beneficial. Carbon monoxide reduces oxygen uptake and delivery and endothelial dysfunction. A systematic review and meta-analysis of studies on preoperative smoking cessation showed a significant difference in PPCs when comparing previous with current smokers (15% vs 20%), with a larger effect seen with a longer duration of abstinence.(54)
Chest physiotherapy, incentive spirometry and deep breathing exercises: is very useful for patients for lung resection procedures and in others at high risk of PPCs. Preoperative chest physiotherapy has been found to be associated with reduced PPCs following major abdominal surgery.(55) Implementation of a perioperative chest physiotherapy program was found to reduce PPCs from 15.5% to 4.7%.(56)
Incentive spirometry can only be effectively used with adequate patient education regarding its use and in the absence of pulmonary physiotherapy. Incentive spirometry has not shown additional advantages than those associated with other manoeuvres such as intermittent positive pressure breathing, deep breathing or noninvasive positive pressure ventilation. (57,58)
In a multidisciplinary patient care programme, postoperative protocol including incentive spirometry, coughing, deep breathing, ambulation, and head-of-bed elevation reduced the incidence of postoperative pneumonia and reintubation following general and vascular surgical procedures. It was also found to result in reduction in rate of pneumonia from 2.6% to 1.6% and the rate of reintubation from 2.0% to 1.2%.(59)
Early ambulation: Specific large body of evidence is not available on effect of early ambulation on PPCs. The evidences so far of the benefit of early ambulation are on the reduced incidence of pulmonary embolism but not on other PPCs.(60,61) Few studies showing reduction in other PPCs are mainly observational and some related to fast track procedures.(62,63,64)
Intravenous fluids and lungs: The shift in favour of volume restriction so that the excessive fluid does not extravasate into the interstitium (including the lungs) has been applied to minimise PPCs in the perioperative period. Thus limiting intraoperative crystalloid volume infusion may decrease PPCs. Many trials have demonstrated reduction of PPCs, shorter times to extubation and hospital length of stay with conservative intravenous fluid regimen compared with a liberal intravenous fluid infusion.(65,66)
Postoperative pulse oximetry: Surprisingly, the theoretical benefits of monitoring oxygenation using pulse oximetry in the post-operative period have not translated to actual evidences of improvements in respiratory outcomes. One trial of more than 20,000 patients showed that perioperative pulse oximetry caused change in the clinical management (including more oxygen and more naloxone), but no reduction in the incidence of PPCs.(67)
Prevention of ventilator-associated pneumonia: The use of specific guidelines for prevention of ventilator assisted pneumonia can be used for prolonges surgeries under GA such as the ‘‘ventilator bundle’’,which consists of elevation of the head of bed, daily sedation disruption with evaluation for extubation potential, peptic ulcer prophylaxis, thromboembolism prophylaxis, and daily oral hygiene with chlorhexidine.(68) Drainage of subglottic secretion and use of closed-circuit suctioning systems are also useful. There are no evidences for the benefit of these measures in the perioperative settings.
Special Group Specific Prevention Strategies
Obstructive lung disease, OSA and obesity, Intrathoracic surgical procedures, Specialized care of ARDS and refractory hypoxia.
Obstructive lung disease: Obstructive lung disease (COPD or asthma) may develop respiratory decompensation due to bronchoconstriction and dynamic hyperinflation (or auto-PEEP) during the perioperative period. Dynamic hyperinflation is primarily caused by inadequate expiratory time to allow lung emptying to reach a normal functional residual capacity. It can be prevented by decreasing the ratio of inspiratory to expiratory time (I:E ratio) i.e. increasing the expiratory time and avoiding tachypnoea.
When there is severe expiratory flow obstruction, a degree of permissive hypercapnoea is allowed. Dynamic hyperinflation may cause PPCs by increasing work-of-breathing. During spontaneous breathing, work-of-breathing can be reduced by application of PEEP and may prevent PPCs. With severe airflow obstruction, inhalation of helium-oxygen (Heliox) can improve airflow.(decreased density and less turbulent flow).
Some patients can be extubated followed by noninvasive positive pressure ventilation (CPAP); this will also prevent reintubation risks; rate of reintubation, pneumonia, and 60-day mortality in ICU patients are reduced.(69)
Intrathoracic procedures: Analgesia has to be a prime consideration so that respiratory mechanics are maintained and thoracoscopy is associated with less pain as compared to open thoracotomies. Epidural analgesia and intercostal nerve blocks are very useful in preventing PPCs following thoracotomies and CABGs. However, use of neuraxial blocks may be restricted by coagulopathy associated with cardiac procedures. Heparin-coated CPB circuits are less proinflammatory and may reduce the risk of lung injury.(70)
Intraoperative haemofiltration to attenuate hypervolemia can reduce PPCs and limiting pulmonary ischemic time during CPB reduces risk of ischemia reperfusion lung injury. Prophylactic CPAP after cardiac surgery can also decrease the incidence of PPCs, including pneumonia and reintubation following cardiac surgery.(71)
Obstructive sleep apnoea and obesity: Noninvasive positive pressure ventilation (such as CPAP), avoidance of sedative premedication, using regional anaesthesia and analgesia. Continuous pulse oximetry for at least 6 hours to demonstrate the absence of significant respiratory events before discharge (72) Avoiding high FiO2 has been associated with improved oxygen saturation and forced expiratory flows in obese patients.(11)
Summary:
The management of the ventilation in the ICUs and in the operation theatres has become more similar with more patients with significant co morbidities undergoing major and prolonged surgeries. The protection of lungs and prevention of pulmonary complications can be achieved by managing the predisposing and causative factors effectively. Ventilation strategies including use of lower tidal volumes,use of PEEP and optimal peak airway pressures ,permissive hypercapnoea and other techniques need to be individualised for each case.
References:
1. J. Kyle Bohman, Daryl J. Kor. Advances in Perioperative Pulmonary Protection Strategies. Advances In Anesthesia. 32 (2014) 89–117
2. Cutler EC, Hunt A. Postoperative pulmonary complications. Arch Surg 1920;1(1): 114–57.
3. Bendixen HH, Hedley-White J, Laver MB. Impaired oxygenation in surgical patients during general anesthesia with controlled ventilation: a concept of atelectasis. N Engl J Med 1963; 96: 156–66
4. Canet J, Gallart L, Gomar C, et al. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology 2010;113(6):1338–50.
5. Dimick JB, Chen SL, Taheri PA, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg 2004;199(4): 531–7
6. Smetana G. Postoperative pulmonary complications: An update on risk assessment and reduction. Cleve Clin J Med 2009; 76: 60–5
7. Khuri SF, Henderson WG, DePalma RG, et al. Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Ann Surg 2005;242(3):326-41[discussion: 341–3].
8. Carney D, DiRocco J, Nieman G. Dynamic alveolar mechanics and ventilator-induced lung
injury. Crit Care Med 2005;33(Suppl 3):S122–8
9. Briel M, Meade M, Mercat A, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA 2010;303(9):865–73.
10. Dos Santos CC. Hyperoxic acute lung injury and ventilator-induced/associated lung injury: new insights into intracellular signaling pathways. Crit Care 2007;11(2):126
11.ZorembaM, Dette F, Hunecke T, et al. The influence of perioperative oxygen concentration on postoperative lung function in moderately obese adults. Eur J Anaesthesiol 2010;27(6): 501–7.
12.Meyhoff CS,Wetterslev J, Jorgensen LN, et al. Effect of high perioperative oxygen fraction on surgical site infection and pulmonary complications after abdominal surgery: the PROXI randomized clinical trial. JAMA 2009;302(14):1543–50.
13.Gajic O, Dara SI, Mendez JL, et al. Ventilator-associated lung injury in patients without acute lung injury at the onset of mechanical ventilation. Crit Care Med 2004; 32: 1817–24
14.Gajic O, Frutos-Vivar F, Esteban A, et al. Ventilator settings as a risk factor for acute respiratory distress syndrome in mechanically ventilated patients. Intensive Care Med 2005; 31: 922–6
15.Michelet P, D’Journo X-B, Roch A, et al. Protective ventilation influences systemic inflammation after esophagectomy: a randomized controlled study. Anesthesiology 2006; 105: 911–9
16.Choi G, Wolthuis EK, Bresser P, et al. Mechanical ventilation with lower tidal volumes and positive end-expiratory pressure prevents alveolar coagulation in patients without lung injury.Anesthesiology 2006; 105: 689–95
17.Determann R, Royakkers A, Wolthuis EK, et al. Ventilation with lower tidal volumes as compared with conventional tidal volumes for patients without acute lung injury: a preventive randomized controlled trial. Crit Care 2010; 14: R1
18.Esther K. Wolthuis, Goda Choi, Mark C. Dessing,Paul Bresser,Rene Lutter, Misa Dzoljic,et al Mechanical Ventilation with Lower Tidal Volumes and Positive End-expiratory Pressure Prevents Pulmonary Inflammation in Patients without Preexisting Lung Injury Anesthesiology 2008; 108:46–54
19.Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. The Acute Respiratory Distress Syndrome Network. N Engl J Med 2000;342(18):1301–8.
20.Serpa Neto A, Cardoso SO, Manetta JA, et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA 2012;308(16):1651–9.
21.Hemmes SN, Serpa Neto A, Schultz MJ. Intraoperative ventilatory strategies to prevent postoperative pulmonary complications: a meta-analysis. Curr Opin Anaesthesiol 2013;26(2):126–33.
22.Ary Serpa Neto, Se´rgio Oliveira Cardoso, Jose´ Antoˆ nio Manetta, Victor Galva˜o Moura Pereira, Daniel Crepaldi Espo´ sito, Manoela de Oliveira Prado Pasqualucci, et al. Association Between Use of Lung-Protective Ventilation With Lower Tidal Volumes and Clinical Outcomes Among Patients Without Acute Respiratory Distress Syndrome: A Meta-analysis. JAMA, October 24/31, 2012—Vol 308, No. 16; 1651-59.
23.Severgnini P, Selmo G, Lanza C, et al. Protective mechanical ventilation during general anesthesia for open abdominal surgery improves postoperative pulmonary function. Anesthesiology 2013;118(6): 1307–21.
24.Imberger G, McIlroy D, Pace NL, et al. Positive end-expiratory pressure (PEEP) during anaesthesia for the prevention of mortality and postoperative pulmonary complications. Cochrane Database Syst Rev 2010;(9):CD007922.
25.Futier E, Constantin JM, Pelosi P, et al. Intraoperative recruitment maneuver reverses detrimental pneumoperitoneum-induced respiratory effects in healthy weight and obese patients undergoing laparoscopy. Anesthesiology 2010;113(6):1310–9.
26.Wolthuis EK, Vlaar APJ, Choi G, Roelofs JJTH, Juffermans NP, Schults MJ. Mechanical ventilation using non-injurious ventilation settings causes lung injury in the absence of pre-existing lung injury in healthy mice. Crit Care 2009; 13: R1
27.Ng CSH, Song Wan, Ho AMH, Underwood MJ. Gene expression changes with a ‘non-injurious’ ventilation strategy. Crit Care 2009; 13: 403
28.Smetana GW, Lawrence VA, Cornell JE. Preoperative pulmonary risk stratification for non cardiothoracic surgery: systematic review for the American College of Physicians. Ann Intern Med 2006; 144(8):581–95.
29.Arozullah AM, Daley J, Henderson WG, et al. Multifactorial risk index for predicting postoperative respiratory failure in men after major noncardiac surgery. The National Veterans Administration Surgical Quality Improvement Program. Ann Surg 2000;232(2): 242–53.
30.Tsiouris A, Horst HM, Paone G, et al. Preoperative risk stratification for thoracic surgery using the American College of Surgeons National Surgical Quality Improvement Program data set: functional status predicts morbidity and mortality. J Surg Res 2012;177(1):1–6.
31.Memtsoudis S, Liu SS, Ma Y, et al. Perioperative pulmonary outcomes in patients with sleep apnea after noncardiac surgery. Anesth Analg 2011;112(1):113–21.
32.Orozco-Levi M, Torres A, Ferrer M, et al. Semirecumbent position protects from pulmonary aspiration but not completely from gastroesophageal reflux in mechanically ventilated patients.Am J Respir Crit Care Med 1995;152 (4 Pt 1):1387–90.
33.Lerman J. On cricoid pressure: ‘‘may the force be with you’’. Anesth Analg 2009;109(5):1363–6.
34.Neilipovitz DT, Crosby ET. No evidence for decreased incidence of aspiration after rapid sequence induction. Can J Anaesth 2007;54(9):748–64.
35.Bice T, Li G, Malinchoc M, et al. Incidence and risk factors of recurrent acute lung injury.Crit Care Med 2011;39(5):1069–73.
36.Safdar N, Crnich CJ, Maki DG. The pathogenesis of ventilator-associated pneumonia: its relevance to developing effective strategies for prevention. Respir Care 2005;50(6):725-39 [discussion:739–41].
37. Li G, Rachmale S, Kojicic M, et al. Incidence and transfusion risk factors for transfusion associated circulatory overload among medical intensive care unit patients. Transfusion. 2011;51(2): 338–43.
38.Triulzi DJ. Transfusion-related acute lung injury: current concepts for the clinician. Anesth Analg 2009;108(3):770–6.
39.Gajic O, Rana R, Winters JL, et al. Transfusion-related acute lung injury in the critically ill: prospective nested case-control study. Am J Respir Crit Care Med 2007;176(9):886–91.
40.Toy P, Gajic O, Bacchetti P, et al. Transfusion-related acute lung injury: incidence and risk factors. Blood 2012;119(7):1757–67.
41.Eder AF, Herron RM Jr, Strupp A, et al. Effective reduction of transfusion-related acute lung injury risk with male-predominant plasma strategy in the American Red Cross (2006-2008). Transfusion 2010; 50(8):1732–42.
42.Koch CG, Li L, Sessler DI, et al. Duration of red-cell storage and complications after cardiac surgery. N Engl J Med 2008;358(12):1229–39.
43.Lee JJ, Kim GH, Kim JA, et al. Comparison of pulmonary morbidity using sevoflurane or propofol-remifentanil anesthesia in an Ivor Lewis operation. J Cardiothorac Vasc Anesth 2012;26(5):857–62.
44.Hofer RE, Sprung J, Sarr MG, et al. Anesthesia for a patient with morbid obesity using dexmedetomidine without narcotics. Can J Anaesth 2005;52(2):176–80.
45.Murphy GS, Szokol JW, Marymont JH, et al. Residual neuromuscular blockade and critical respiratory events in the postanesthesia care unit. Anesth Analg 2008;107(1):130–7.
46.Kumar GV, Nair AP, Murthy HS, et al. Residual neuromuscular blockade affects postoperative pulmonary function. Anesthesiology 2012;117(6):1234–44.
47.Plaud B, Debaene B, Donati F, et al. Residual paralysis after emergence from anesthesia. Anesthesiology 2010;112(4):1013–22
48.Wahba WM, Don HF, Craig DB. Post-operative epidural analgesia: effects on lung volumes.Can Anaesth Soc J 1975;22(4):519–27
49.Macfarlane AJ, Prasad GA, Chan VW, et al. Does regional anesthesia improve outcome after total knee arthroplasty? Clin Orthop Relat Res 2009;467(9):2379–402.
50.Liu SS, Block BM,Wu CL. Effects of perioperative central neuraxial analgesia on outcome after coronary artery bypass surgery: a meta-analysis. Anesthesiology 2004;101(1): 153–61.
51.Memtsoudis SG, Sun X, Chiu YL, et al. Perioperative comparative effectiveness of anesthetic technique in orthopedic patients. Anesthesiology 2013;118(5):1046–58.
52.Stundner O, Rasul R, Chiu YL, et al. Peripheral nerve blocks in shoulder arthroplasty: how do
they influence complications and length of stay? Clin Orthop Relat Res 2014;472(5): 1482–8.
53.Wiesmann T, Steinfeldt T,Wagner G, et al. Supplemental single shot femoral nerve block for total hip arthroplasty: impact on early postoperative care, pain management and lung function.Minerva Anestesiol 2014;80(1):48–57.
54.Mills E, Eyawo O, Lockhart I, et al. Smoking cessation reduces postoperative complications:
a systematic review and meta-analysis. Am J Med 2011;124(2):144–54.e8.
55.Pouwels S, Stokmans RA, Willigendael EM, et al. Preoperative exercise therapy for elective major abdominal surgery: a systematic review. Int J Surg 2014;12(2):134–40
56.Novoa N, Ballesteros E, Jimenez MF, et al. Chest physiotherapy revisited: evaluation of its influence on the pulmonary morbidity after pulmonary resection. Eur J Cardiothorac Surg 2011;40(1):130–4
57.do Nascimento P Jr, Modolo NS, Andrade S, et al. Incentive spirometry for prevention of postoperative pulmonary complications in upper abdominal surgery. Cochrane Database Syst Rev 2014;(2):CD006058.
58.Overend TJ, Anderson CM, Lucy SD, et al. The effect of incentive spirometry on postoperative pulmonary complications: a systematic review. Chest 2001;120(3):971–8.
59.Cassidy MR, Rosenkranz P, McCabe K, et al. I COUGH: reducing postoperative pulmonary complications with a multidisciplinary patient care program. JAMA Surg 2013;148(8):740–5.
60.White RH, Gettner S, Newman JM, et al. Predictors of rehospitalization for symptomatic venous thromboembolism after total hip arthroplasty. N Engl J Med 2000;343(24):1758–64.
61.Geerts WH, Heit JA, Clagett GP, et al. Prevention of venous thromboembolism. Chest 2001;119(Suppl 1):132S–75S.
62.Haines KJ, Skinner EH, Berney S. Association of postoperative pulmonary complications with delayed mobilisation following major abdominal surgery: an observational cohort study. Physiotherapy 2013;99 (2):119–25.
63.Rawal N, Sjostrand U, Christoffersson E, et al. Comparison of intramuscular and epidural morphine for postoperative analgesia in the grossly obese: influence on postoperative ambulation and pulmonary function. Anesth Analg 1984;63(6):583–92.
64.Kamel HK, Iqbal MA, Mogallapu R, et al. Time to ambulation after hip fracture surgery: relation to hospitalization outcomes. J Gerontol A Biol Sci Med Sci 2003;58(11): 1042–5.
65.Nisanevich V, Felsenstein I, Almogy G, et al. Effect of intraoperative fluid management on outcome after intraabdominal surgery. Anesthesiology 2005;103(1):25–32.
66.Kita T, Mammoto T, Kishi Y. Fluid management and postoperative respiratory disturbances in patients with transthoracic esophagectomy for carcinoma. J Clin Anesth 2002;14(4): 252–6.
67.Moller JT, JohannessenNW, Espersen K, et al. Randomized evaluation of pulse oximetry in 20,802 patients: II. Perioperative events and postoperative complications. Anesthesiology 1993;78(3):445–53.
68.Institute for Healthcare Improvement. Implement the IHI ventilator bundle. 2014. Available at: http://www.ihi.org/resources/Pages/Changes/ImplementtheVentilatorBundle.aspx. Accessed on 30 Nov 2014
69.Ferrer M, Esquinas A, Arancibia F, et al. Noninvasive ventilation during persistent weaning failure: a randomized controlled trial. Am J Respir Crit Care Med 2003;168(1):70–6.
70.Redmond JM, Gillinov AM, Stuart RS, et al. Heparin-coated bypass circuits reduce pulmonary injury. Ann Thorac Surg 1993;56(3):474–8 [discussion: 479].
71.Zarbock A, Mueller E, Netzer S, et al. Prophylactic nasal continuous positive airway pressure following cardiac surgery protects from postoperative pulmonary complications: a prospective, randomized, controlled trial in 500 patients. Chest 2009;135(5):1252–9.
72.Porhomayon J, Nader ND, Leissner KB, et al. Respiratory perioperative management of
patients with obstructive sleep apnea. J Intensive Care Med 2014;29:145–53.