Conference Lectures
Dr. Mallikarjuna D
POST DURAL PUNCTURE HEADACHE IN PARTURIENTS
- INTRODUCTION
Post-Dural puncture headache (PDPH) was first described by August Bier in 1898 and classically presents as a postural headache following therapeutic or diagnostic interventions of the epidural or spinal space.
The incidence of PDPH is estimated to be between 30-50% following diagnostic or therapeutic lumbar puncture, 0-5% following spinal anaesthesia and up to 81% following accidental dural puncture during epidural insertion in the pregnant woman.
According to the International Headache Society, the criteria for PDPH include a headache that develops less than seven days after a spinal puncture, occurs or worsens less than fifteen minutes after assuming the upright position, and improves less than thirty minutes in the recumbent position with at least one of the following (neck stiffness, tinnitus, hyperacusia, photophobia, and nausea). The headache should disappear within fourteen days after a spinal puncture; if it persists, it is called a CSF fistula headache.
- ANATOMY AND PATHOGENESIS
Anatomically, the spinal dura mater extends from the foramen magnum to the second segment of the sacrum. It consists of dense connective tissue matrix of collagen and elastic fibers. The average adult produces about 500 mL of CSF per day, or 21 mL per hour (0.3 mL/kg/hr), with 90% coming from the choroid plexus, and 10% from the brain substance itself. A total of about 150 mL of CSF circulates at any one time and is absorbed by arachnoid villi. The cause of PDPH is not entirely certain. The best explanation is that low CSF pressure results from CSF leakage through a dural and arachnoid tear; a leakage that exceeds the rate of CSF production. As little as 10% loss of CSF volume can cause an orthostatic headache. There are two basic theoretical mechanisms to explain PDPH. One is reflex vasodilatation of the meningeal vessels due to the lowered CSF pressure. The other is the traction on the pain sensitive intracranial structures in the upright position. The traction on the upper cervical nerves like C1, C2, C3 causes the pain in the neck and shoulders. Traction on the fifth cranial nerve causes the frontal headache. Pain in the occipital region is due to the traction of the ninth and tenth cranial nerves
- RISK FACTORS
Women, particularly during pregnancy and especially after vaginal delivery, are considered at increased risk for PDPH. The incidence of PDPH is highest between 18 and 30 years of age and declines in children younger than 13 years and adults older than 60 years. The incidence is greater in patients with lower body mass index. Women who are obese or morbidly obese may actually have a decreased incidence of PDPH. This may be because the increase in intra-abdominal pressure may act as an abdominal binder helping to seal the defect in the dura and decreasing the loss of CSF. Younger women may be at a greater risk because of increased dural fiber elasticity that maintains a patent dural defect compared to a less elastic dura in older patients. Patients with a headache before lumbar puncture and a prior history of PDPH are also at increased risk.
Other risk factors include,
- Equipment-related factors(type, size and shape)
The most widely used spinal needles include the Tuohy, Sprotte, Quincke, Whitacre, and Atraucan needles.The Tuohy large bore 16- or 18-gauge epidural catheters were used for spinal anesthesia and have an opening at the end of the needle and a curved tip intended to prevent dural puncture. Atraucan and Quincke needles are similar in that they have an opening at the end of the needles and a sharp cutting tip. In contrast, Sprotte and Whitacre needles have a broader tip and an opening close to, but not at the end of the needle.
- Procedure -related factors(bevel orientation, angle of insertion and stylet replacement)
Procedure-related risk factors for post-Dural puncture headache
RISK FACTORS FOR PDPH |
INCIDENCE OF PDPH |
COMMENT |
RECOMMENDATION |
|
Needle size |
Gauge of quincke needle |
|
Incidence of PDPH decreases with the use of higher gauge needles keeping the needle type constant |
|
22G |
36% |
|||
25G |
25% |
|||
26G |
2-12% |
|||
>26G |
<2% |
|||
Needle shape and type |
22G whitacre |
3% |
|
A traumatic needles |
|
22G quincke |
36% |
||
22G sprotte |
12.2% |
|||
22G quincke |
24.4% |
|||
Needle orientation |
parallel/narrow angle |
10.9% |
This technique is likely less important in reducing the incidence of PDPH with |
Bevel parallel to the long axix of the spine/angle should be narrow |
perpendicular/angle not arrow |
25.8% |
|||
Stylet reinsertion |
Stylet re-inserted |
5% |
|
Reinsert stylet prior to removal of the needle |
Stylet not re-inserted |
16.3% |
|||
Operator experience |
Experience(# of epidurals administered) |
|
Finding of higher PDPH incidence in resident may be confounded by fatigue |
Better trained residents cause fewer accidental dural punctures |
<10 |
2.5% |
|||
10-29 |
2.0% |
|||
30-59 |
1.4% |
|||
>60 |
1.2-1.3% |
|||
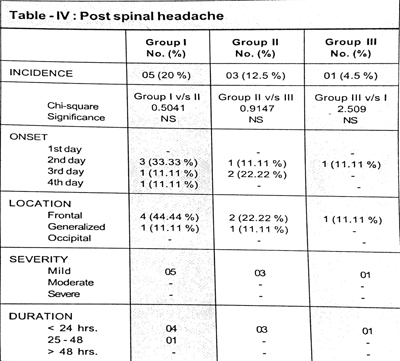
Group I : Patients who received spinal anaesthesia with
25 gauge quincke needle.
Group II : Patients who received spinal anaesthesia with
27 gauge quincke needle.
Group III : Patients who received spinal anaesthesia with
27 gauge whitacre needle.
(Indian J. Anaesth. 2002; 46 (5) : 373-377 : PDPH IN C)
- CLINICAL FEATURES
The cardinal features of PDPH as defined by the International Headache Society are a headache that develops within 7 days of Dural puncture and disappears within 14 days; however PDPH has been reported to occur later and continue for longer than the times. Classic features of the headache caused by dural puncture are listed below but presentation is often variable.
- Headache is often frontal-occipital.
- Most headaches do not develop immediately after dural puncture but 24-48 hours after the procedure with 90% of headaches presenting within 3 days.
- The headache is worse in the upright position and eases when supine.
- Pressure over the abdomen with the woman in the upright position may give transient relief to the headache by raising intracranial pressure secondary to a rise in intra-Abdominal pressure (Gutsche sign).
Associated symptoms that may be present include neck stiffness, photophobia, tinnitus, visual disturbance and cranial nerve palsies.
- MANAGEMENT
1. Conservative Management
Most post-Dural puncture headaches will resolve spontaneously. Conservative management has traditionally involved bed rest and fluids though there is little evidence to support either of these measures. A recent Cochrane review concluded that routine bed rest after dural puncture is not beneficial and should be abandoned. While routine administration of additional fluids may be unnecessary, avoidance of dehydration is advisable to help limit headache severity.
2. Pharmacological
Simple analgesia should be instituted in all patients with PDPH; regular paracetamol and non-steroidal anti-inflammatory medications (if tolerated) may control symptoms adequately.
Caffeine
Caffeine was first reported as a treatment for PDPH in 1949. Caffeine is a central nervous system stimulant and is thought to influence PDPH by inducing cerebral vasoconstriction. Doses from 75 –500 mg have been investigated and caffeine has been administered orally, intramuscularly and intravenously.
Synacthen (synthetic ACTH)
Synthetic ACTH was first reported to be effective for treating PDPH in the 1990s. Postulated mechanisms include CSF retention through increased mineralocorticoid mediated sodium reabsorption, and a direct analgesic effect via its glucocorticoid activity. Most reports of its effectiveness stem from case reports and case series; however a randomised controlled trial in 2004 found no effect of a single
intramuscular injection of Synacthen compared with an intramuscular injection of normal saline. It is unknown whether a larger or repeated dose of Synacthen may be beneficial.
Other Drugs
Numerous other reports exist in the literature with promising results for a variety of other pharmacological agents including: 5HT agonists (e.g.sumatriptan), gabapentin, DDAVP, theophyline, and hydrocortisone. To date there is insufficient evidence to support their use.
INVASIVE MANAGEMENT
Epidural blood patch (EBP)
After the (probably erroneous) observation that patients who had a bloody spinal tap at lumbar puncture were less likely to develop PDPH, the first epidural blood patch was performed in 1960 by the American surgeon, Dr James Gormley. Just 2 ml of the patient’s blood was injected during the first epidural blood patch and the headache was relieved. Epidural blood patching involves injection of autologous blood into the epidural space. It remains one of the few proven treatments of PDPH however the mechanism of action remains unclear. The resulting blood clot may have a “patch effect” on the dural tear while the volume of blood transfused into the epidural space raises intracranial pressure and reduces ongoing CSF leak. Despite the early successes and long history of the epidural blood patch a number of controversies exist regarding the technique including its true effectiveness, the best technique and its safety.
Effectiveness
- Early studies of the efficacy of EBP (up to 90%) were overstated probably because of inadequate patient follow up and inclusion of patients who had PDPH resulting from dural puncture by different types and gauge of needles. Reported success rates have fallen over time and current data suggest that permanent cure by a single blood patch can be expected in 50% of patients.
- About 40% of patients require a second blood patch.
- Despite the falling success rates, EBP remains the most effective treatment for PDPH and has been shown in a randomised controlled trial to be more effective than conservative treatment in treating established PDPH.
Optimal Technique
- EBP should be performed by two personnel, one an experienced anaesthetist, the other competent in taking a volume of blood from the arm. Both should employ full aseptic precautions.
- Contraindications to EBP include: sepsis, coagulopathy and patient refusal.
- EBP is likely to be most effective if performed at least 24 hours after the onset of PDPH.
- Volumes of between 2-60mls of blood have been used. Optimal volume is unknown but current recommendations suggest 10 to 20ml should be injected. If the patient reports discomfort in the back during the procedure the injection should be stopped.
- The patient should lie flat for 1-2 hours after the procedure. There is no evidence that bed rest for longer than this time is beneficial.
- Once discharged from hospital, follow up by telephone over the first few days after EBP and review at 6 weeks is sensible.
Safety
- Strict asepsis must be maintained during epidural blood patching.
- EBP should not be performed in the presence of leucocytosis or fever due to the risk of meningitis.
- Minor complications include backache, neckache and transient bradycardia.
- Major complications of epidural blood patching, although rare, may occur and include:
- Meningitis, subdural haematoma, seizures, arachnoiditis, spastic paraparesis, dural puncture, cauda equina syndrome.
- Epidural blood patch may be unacceptable to some Jehovah’s Witness patients.
- Clinicians should discuss the risks and benefits of an epidural blood patch with individual patients.
- If an epidural blood patch fails to relieve a PDPH, it may be prudent to consider radiological imaging of the head to exclude other pathology prior to repeating the blood patch.
Prophylactic Epidural Blood Patch
A potentially attractive option in the face of a recognized dural puncture with a Tuohy needle is to resite the epidural so that a prophylactic epidural blood patch (PEBP) can be provided in the hope of preventing a subsequent PDPH. The popularity of this technique has diminished recently for a number of reasons including the limited evidence that PEBP reduces the requirement for a therapeutic EBP, the increasing use of intrathecal catheter placement following dural puncture which may itself reduce the risk of subsequent PDPH and the recognition that some dural punctures don’t result in a PDPH and many PDPHs do not require a therapeutic EBP. Administering a PEBP to patients following dural puncture may therefore expose these patients to an unnecessary procedure with associated risks.
Epidural Fluids
A number of fluids, both crystalloids and colloids have been infused in to the epidural space. Fluid infusion may increase the CSF pressure and provide temporary relief of the headache. Longer term relief is less likely and the long term effect of colloid particles in the epidural space is unknown.
Epidural Morphine
A number of authors have advocated the use of epidural opioids for the treatment and prophylaxis of PDPH. A recent small randomized study found that 3mg epidural morphine reduced the development of PDPH and need for EBP following inadvertent dural tap. Larger trials of this therapy are awaited.
- PREVENTION
Spinal Needle Selection
Smaller gauge spinal needles with pencil point tips such as the Whitacre and Sprotte needle are associated with lower rates of PDPH. Pencil point needles part rather than cut the dural fibres, and so the hole in the dura closes more quickly. Ideally, spinal needles no larger than 25G should be used.
