Conference Lectures
Ultrasound guided Lower limb nerve blocks: Video session
Dr.R. Manikandan, MD. Ganga Hospital, Coimbatore.
The practice of regional anesthesia requires a sound understanding of anatomy.In orderto practice safe and successful lower extremity regionalanesthesia, a fundamental understanding of the lumbarplexus and sacral plexus is necessary.
Relevant anatomy
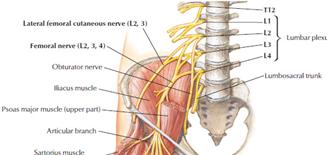
The lumbar plexus innervates muchof the skin and subcutaneous tissue (dermatomes),muscle (myotomes), and bones (osteotomes) of thelower abdominal wall, pelvis, genitalia, and the medialand anterior aspects of the thigh. It primarily arisesfrom the ventral rami of the L1 through L4 spinalnerves, with occasional contribution from the T12and/or L5 segments as well. The plexus forms in theposterior abdominal wall anterior to the transverseprocesses of the vertebrae, deep within the psoas muscle.As it travels distally, the lumbar plexus quickly beginsto give off branches to the surrounding musculatureand begins to divide into some of the terminalnerves as the Iliohypogastric, Ilioinguinal, and genitofemoral nerves (L1 - L2). The lumbarplexus then divides into an anterior division, fromwhichthe obturator nerve (L2 - L4) arises, and a posteriordivision, from which the femoral (L2 - L4)and lateral femoral cutaneous nerves (L2- L3) arise.
![]()
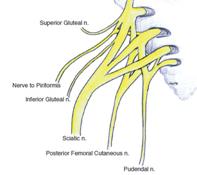
The sacral plexus innervates much ofthe skin and subcutaneous tissue,muscle and bones of thegluteal, pelvic, posterior thigh, and much of the legregions. It arises from the ventral rami of the L4through S4 spinal nerves, as the lumbosacral trunk(L4 and L5) descends along the medial border of thepsoas major muscle to join the sacral plexus at theS1 level. The plexus travels near the posterior wall ofthe pelvis towards the greater sciatic foramen. Along itscourse, the sacral plexus gives off branches to thesurrounding musculature (gluteus maximus/minimus,quadratus femoris, obturator internus, piriformis, levatorani, and external anal sphincter muscles), as well asthe pudendal nerve (S2 - S4), which providesinnervation to the skin and muscles of the perineum and the posterior cutaneous nerve of thethigh (S1 - S3), which supplies cutaneous sensationto the posterior aspect of the thigh and leg.The sacral plexus then continues as the sciatic nerve(L4 - S3), its main terminal nerve, through thegreater sciatic foramen into the gluteal region.
Major nerves and block techniques.
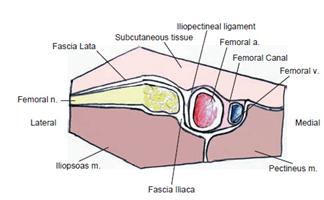
The femoral nerve travels lateralto the psoas major muscle and passes under theinguinal ligament with the femoral artery andvein, lateral to the vessels, into the anterior thigh.It provides muscle innervation along its pathand, once in the thigh, divides into many branchesto provide muscle innervation to many of the muscles of the anterior thigh.
The ultrasound-guided femoral nerve block is a relatively simple block to perform, but useful in multiple clinical settings. It can be used to supply anesthesia to the anterior thigh and knee, or to supply analgesia for femur and knee surgery, as well as hip procedures.
Technique
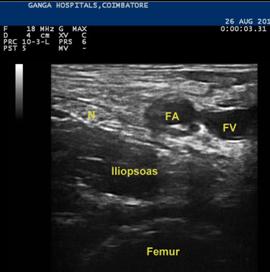
The patient should be positioned supine with his/herarms resting comfortably across his/her chest or stomach. A wide, sterile preparation is applied to the inguinalregion, and sufficient ultrasound gel is applied to thesite or probe to ensure adequate imaging.The ultrasound probe is positioned along thetransverse plane near theinguinal crease. Thiswill yield an ultrasound image in the transverse planeto the target structures. The orienting structure to perform this block is the femoral artery. At the site where thescanning and procedure are performed, the ultrasoundimage will show the femoral nerve locatedimmediately lateral to the femoral artery, and justmedial to the iliopsoas muscle. The femoral vein islocated medial to the femoral artery.
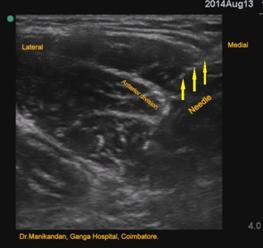
Once an adequate image has been obtained, a skin wheal israised with local anesthetic at the lateral end of theultrasound probe. A blunt-tipped needle is placedthrough the wheal and advanced in-plane withthe ultrasound beam in a lateral to medial direction,posteriorly towards the femoral nerve. Underthe transducer, the needle is visible as a hyperechoicline.
![]()


The path of theneedle should be aimed just lateral to the femoral nerve and careshould be taken to avoid contacting the nerve, in order tominimize the potential for nerve damage. Once the needle is positioned in the ideal initiallocation, and initial negative aspiration of blood isconfirmed, the injection of local anesthetic canbegin. If there is high resistance toinjection, stop and reposition the needle. Pay specialattention to the spread of the local anesthetic, whichwill appear as an expanding hypoechoic region. The ideal spread shouldbe circumferential around the femoral nerve. A total volume of 20ml of local anesthetic (bupivacaine or ropivacaine) at desired concentration can be injected.
Obturator nerve block
The obturator nerve travels medial to the psoas major muscle andpasses through the obturator canal with theobturator vessels into the medial aspectof the thigh. Here it divides into an anterior and posterior branch that continue to supply severalof the muscles along the medial thigh primarilyinvolved in adduction of the thigh, as well asflexion and extension of the thigh. It supplies cutaneous sensation to the medialaspect of the thigh as the medial femoral cutaneousnerves, and provides sensation to the hip jointand the medial aspect of the knee joint
 .
.
The anterior and posterior divisions of the obturator nerve converge proximally along therounded lateral border of the adductor brevis muscle. The obturator nerve divisions are thinand flat as the fascicles disperse to the muscle groups. The obturator nerve divisions have a“white bands” appearance on sonography.Therefore, theobturator nerve block is usually performed as a multiple-injection technique targeting eachof the two divisions separately.The block is performed in supine position with the leg slightly abducted. The obturatordivisions and adductor brevis are visualized in short-axis view in the medial thigh. This isbest accomplished by sliding the transducer between proximal and distal locations to observethe convergence of the divisions along the lateral border of the adductor brevis. An out-ofplaneapproach is often used because of the proximity of the femoral vessels to the needlepath for an in-plane approach.Care is taken to avoid puncture ofthe adjacent obturator arteries because puncture of these vessels can cause haemorrhage.

Sciatic Nerve Block
The sciatic nerve is created by the combination ofthe common peroneal nerve (L4 through S2) with thetibial nerve (L4 through S3). It travels out of theposterior pelvis, through the greater sciatic foramen,into the gluteal region. Here, it passes lateral to theischial tuberosity, in the fascial plane between thegluteus maximus (superficially) and obturator internus(deeply) muscles, as it enters the posterior thigh.Once in the thigh it travels posterior to the femurwithin the “sciatic groove” formed by the bicepsfemoris (laterally) and semitendinosus and semimembranosus(medially) muscles, toward the poplitealfossa. Along its path, the sciatic nerve innervates theadductor magnus, biceps femoris, semitendinosus,and semimebranosus muscles that aid in adductionand flexion of the thigh, as well as flexion of the knee.When thesciatic nerve enters the popliteal fossa, on the posterioraspect of the knee, it separates into the common peronealand tibial nerves.
Techniques
The sciatic nerve can be blocked using ultrasoundfrom numerous positions along its course into the thigh and knee.
Popliteal approach
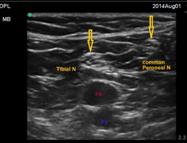
The ultrasound-guided lateral popliteal fossa block ofthe sciatic nerve is a regional anesthetic approach forsurgical procedures of the distal leg, foot, and ankle.This technique is performed at the most cephaladportion of the popliteal fossa or around the distalthird of the thigh near the bifurcation of the sciaticnerve into its two branches. The patient is placed in lateral or prone position to expose the popliteal fossa. The popliteal artery is identified at thestarting position near the popliteal apex using a high frequency linear probe. The nerveis typically found lateral and posterior relative to theartery, and may appear as separate tibialand common peroneal nerve components at thisdistal location.By scanning away from the poplitealspace proximally, keeping the nerve(s) in view , the biceps femoris muscle is identified. The muscle bellyis anatomically lateral and posterior to the sciaticnerve. The branching location of thecommon peroneal and tibial nerves may also be identifieddepending on the patient’s anatomy.At the mid-distal thigh position, the sciaticnerve typically lies within a fascial plane thatseparates the hamstring muscles and appears as around ball structure. The nerve willcharacteristically exhibit anisotropy.The block needle should be placed in proximity tothe nerve to pierce the surrounding fascia, withoutactually entering the nerve. Injection should be given in 3- to 5-ml increments withaspirations attempted in between to ensurethe needle tip remains extravascular. 15 to 20ml of Local anesthetic is sufficient for the block.


Subgluteal approach
To image the pertinent structures for thistechnique, the patient is placed in the lateral positionwith the side to be blocked facing up. The hips andnon-dependent knee are slightly flexed to increase clarityof the patient’s surface anatomy. A curvilinear low frequency transducer is placed atthe midpoint of an imaginary line connecting thepatient’s greater trochanter and ischial tuberosity onthe side to be blocked. An ultrasound image of this area appears essentiallyas 2 layers of muscle separated by fascia. The bonylandmarks (greater trochanter and ischial tuberosity),on either side, appear to hold these muscle layers inplace. Skin and subcutaneous tissue lie atop the mostsuperficial layer: the gluteus maximus muscle. The gluteus maximus muscle has a striped texture typical ofthe mixed echogenicity of muscle. This muscle layer isseparated fromthe quadratus femoris muscleby fascial planes that overlay the bodies of the musclebellies. These fascial planes are hyperechoic and extendfrom the top of the greater trochanter to the ischialtuberosity when imaged in cross-section.The sciatic nerve typically lies within this fascial plane,midway between the greater trochanter and the ischialtuberosity, and appears as a hyperechoic oval structure. Use of a nerve stimulator to aid confirmation of thesciatic nerve’s location can be useful when first learningthis technique, or in cases where difficulty isencountered visualizing the nerve.Needle positioning is undertaken with a blunttippedblock needle introduced through the skin whealusing an in-plane approachAn out-of-plane (OOP) approach to the nerve may also be used for this block for easier needle manipulationand shorter needle distance to the target from thepoint of insertion.


Lateral Femoral Cutaneous nerve block.
 The lateral femoral cutaneous nerve travels laterally from the psoas major muscle,along the iliacus muscle, towards the anteriorsuperior iliac spine (ASIS) and passes under thelateral portion of the inguinal ligament. Here itsupplies cutaneous sensation along the lateralaspect of the thigh down to the knee. High-resolution ultrasound imaging can identify the LFCN superficial to the Sartorius muscle in the proximal thigh. The nerve has a characteristic medial to lateral course overthis muscle. The nerve and muscle are best visualized just medial and distal to the ASIS.The best imaging technique is to slide the transducer along the known courseof the nerve with the nerve viewed in short axis.Rather than passing overthe sartorius, in some patients the LFCN can pass through the sartorius muscle (Incidence 3% - 22%).The sartorius muscle is imaged in shortaxisview near its insertion on the ASIS. By sliding the ultrasound transducer back and forthbetween proximal and distal locations, the LFCN is identified by its characteristic lateralcourse over the sartorius muscle. The in-plane approach can be used from the lateral aspectof the thigh.
The lateral femoral cutaneous nerve travels laterally from the psoas major muscle,along the iliacus muscle, towards the anteriorsuperior iliac spine (ASIS) and passes under thelateral portion of the inguinal ligament. Here itsupplies cutaneous sensation along the lateralaspect of the thigh down to the knee. High-resolution ultrasound imaging can identify the LFCN superficial to the Sartorius muscle in the proximal thigh. The nerve has a characteristic medial to lateral course overthis muscle. The nerve and muscle are best visualized just medial and distal to the ASIS.The best imaging technique is to slide the transducer along the known courseof the nerve with the nerve viewed in short axis.Rather than passing overthe sartorius, in some patients the LFCN can pass through the sartorius muscle (Incidence 3% - 22%).The sartorius muscle is imaged in shortaxisview near its insertion on the ASIS. By sliding the ultrasound transducer back and forthbetween proximal and distal locations, the LFCN is identified by its characteristic lateralcourse over the sartorius muscle. The in-plane approach can be used from the lateral aspectof the thigh.
Adductor canal block (Saphenous nerve block)
The saphenous nerve is a sensory branch of the femoral nerve that travels with the superficialfemoral artery in the thigh along with the infrapatellar nerve and a nerve to the vastusmedialis.Under the sartorius muscle, this complex forms the subsartorial plexus, which alsocan include contributions from the posterior division of the obturator nerve. Saphenous nerve block can be performed in the mid-thigh with the patient in the supineposition. An in-plane approach from the anterior thigh can be used to direct the needle tipthrough the sartorius muscle. A volume of 10 -15ml of local anesthetic is sufficient for this block.


Suggested reading
- Ultrasound-Guided Regional Anesthesia. A Practical Approach to Peripheral Nerve Blocks and Perineural Catheters. Fernando L. Arbona, Babak Khabiri, John Norton.
- Atlas of Ultrasound-GuidedRegional Anesthesia. 2nd Edition. Andrew T. Gray.