| ANAESTHESIA PEARLS | |||||||
|







| Anaphylaxis during general anaesthesia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Death or permanent disability from anaphylaxis in anaesthesia may be avoidable if the reaction is recognised early and managed optimally | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recognition of anaphylaxis during anaesthesia is usually delayed because key features such as hypotension and bronchospasm more commonly have a different cause. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| If anaphylaxis is suspected during anaesthesia, it is the anaesthetist’s responsibility to ensure the patient is referred for investigation. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Anaphylaxis is a severe, life-threatening, generalized or systemic hypersensitivity reaction. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The following guidelines to be applied in suspected anaphylactic reactions associated with anaesthesia. 2007 Scandinavian Clinical Practice Guidelines, the 2008 Resuscitation Council UK guidelines and the British Society for Allergy & Clinical Immunology (BSACI) guidelines. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Causes | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Individuals with a history of atopy, asthma or allergy to some foods appear to be at increased risk of latex allergy. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Patients with asthma or taking b-blocking drugs may suffer a more severe reaction. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Antibiotics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Chlorhexidine | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Dextran | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Gelatins | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hydroxyethylstarch (HAES) | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Iodinated contrast media | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ketamine | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Natural rubber latex | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Local anaesthetics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Midazolam | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Neuromuscular blocking agents (NMBAs) - The quaternary ammonium ion is identified as the allergenic epitope, and is shared by all NMBAs, morphine, pholcodine and other morphine/codeine analogues. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Opioids - Morphine, codeine and meperidine | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Propofol | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Thiopental | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Symptoms and diagnosis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cutaneous symptoms, such as flushing, urticaria and oedema, are common, but, during anaesthesia, these are usually hidden by surgical drapings. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hypotension and tachycardia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severe arrhythmias and cardiovascular collapse if not recognised and treated. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bronchospasm | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cardiovascular collapse | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Bronchospasm | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Transient | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Asthmatics | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cutaneous Rash | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Erythema | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Urticaria | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Angioedema | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Generalised oedema | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Pulmonary oedema | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Classification of clinical manifestations of anaphylaxis during anaesthesia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Scandinavian Society of Anaesthesiology and Intensive Care Medicine (SSAI ) Guideline on treatment of anaphylactic reactions during anaesthesia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
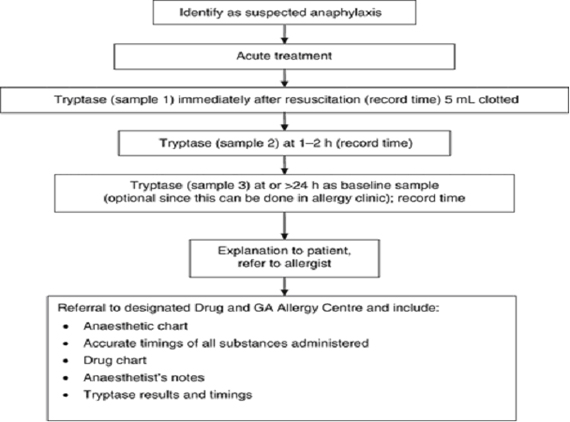
| BSACI guidelines for the investigation of suspected anaphylaxis during general anaesthesia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| SUSPECTED ANAPHYLACTIC REACTIONS ASSOCIATED WITH ANAESTHESIA | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The Association of Anaesthetists of Great Britain and Ireland and British Society for Allergy and Clinical Immunology | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Scandinavian Clinical Practice Guidelines on the diagnosis, management and follow-up of anaphylaxis during anaesthesia† | GUIDELINES | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Suspected Anaphylactic Reactions Associated with Anaesthesia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Association of Anaesthetists of Great Britain and Ireland | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interestingly contradicting case reports | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severe Anaphylactic Shock with Methylene Blue Instillation | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| A 30-yr-old woman was scheduled for surgical correction of tubal sterility. She did not suffer from any atopy. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| After 1 h of uneventful anesthesia (midazolam, sufentanil, propofol, atracurium) and surgery,an intrauterine 1% methylene blue instillation was administered to verify tubal permeability. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Within 2 min after methylene blue instillation,there was a marked decrease in Spo2 to less than 80% and an end-tidal carbon dioxide concentration (18 mm Hg) together with a decrease in arterial blood pressure (60/26 mm Hg) associated with a tachycardia (140 bpm). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| At the same time, the patient developed a severe bronchospasm. All these symptoms were relieved by titrated epinephrine injections (total dose, 1.8 mg), intravascular fluid administration, salbutamol spray, and 40 mg methylprednisolone. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| When hemodynamic stability was restored, a generalized urticaria became apparent. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The patient continued to require epinephrine for 18 h to maintain cardiovascular stability but was discharged home after a few days without sequelae. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Plasma histamine level measured to confirm onset of histamine release was markedly increased to 700 nmol/L (normal 10 nmol/L). | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Six weeks later cutaneous tests to methylene blue was positive whereas cutaneous tests to latex and to all other drugs were negative. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| To confirm the responsibility of methylene blue, in vitro leukocyte histamine release assay (3) was performed with methylene blue and was positive. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Interestingly, methylene blue inhibits guanylate cyclase, thus decreasing cyclic guanosine monophosphate and vessel relaxation in vascular smooth muscle, and it has therefore been proposed for use in hypotensive septic shock patients or as a lifesaving alternative drug for contrast-medium induced anaphylaxis to restore arterial blood pressure. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ref: |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Severe Anaphylactic Shock with Methylene Blue Instillation A & A July 2005 vol. 101 no. 1 149-150 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene blue for clinical anaphylaxis treatment: a case report | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| A 23-year-old female suddenly presented urticaria and pruritus, initially on her face and arms, then over her whole body. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Oral antihistamine was administered initially, but without improvement in symptoms and signs until intravenous methylprednisolone 500 mg. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Recurrence occurred after two hours, plus vomiting. Associated upper respiratory distress, pulmonary sibilance, laryngeal stridor and facial angioedema (including erythema and lip edema) marked the evolution. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| At sites with severe pruritus, petechial lesions were observed. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The clinical situation worsened, with dyspnea, tachypnea, peroral cyanosis, laryngeal edema with severe expiratory dyspnea and deepening unconsciousness. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Conventional treatment was ineffective. Intubation and ventilatory support were then considered, because of severe hypoventilation. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| But, before doing that, based on their previous experience, 1.5 mg/kg (120 mg) bolus of 4% MB was infused, followed by one hour of continuous infusion of another 120 mg diluted in dextrose 5% in water. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Following the initial intravenous MB dose, the clinical situation reversed completely in less than 20 minutes, thereby avoiding tracheal intubation. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Previously the same team has treated nine patients who developed anaphylactic shock and/or anaphylaxis with an intravenous bolus of methylene blue (1.5 to 2.0 mg/kg) treatment. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| These observations do not allow it to be assumed that methylene blue would be the first-choice drug for anaphylactic shock. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ref: |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene blue for clinical anaphylaxis treatment: a case report Sao Paulo Med. J. vol.125 no.1 São Paulo Jan. 2007 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene Blue revisited | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene blue was identified by Paul Ehrlich about 1891 as a successful treatment for malaria. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene Blue was till now known mainly as a dye but is now entering into the field of cardiac surgery and critical care as a very important therapeutic agent with diverse applications. Methylene blue, an inhibitor of nitric oxide synthase and guanylate cyclase has many uses in medicine. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| It has been found to improve the hypotension associated with various clinical states like septic shock, Vasoplegic syndrome and hepatopulmonary syndrome. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Physiology: The enzyme Guanylyl cyclase synthesizes cGMP. In smooth muscle, cGMP is the signal for relaxation, and is coupled to many homeostaic mechanisms including regulation of vascular and airway tone. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene Blue acts by inhibiting guanylate cyclase, thus decreasing C-GMP and vascular smooth muscle relaxation. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| It helps Methylene Blue to improve hypotension in anaphylaxis by decreasing vascular smooth muscle relaxation. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene blue does not interfere with Nitric Oxide release (not interfere with bronchospasm) but acts to block its action on vascular smooth muscles. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The evidence for its use in methemoglobinemia is well established but that for its use in vasoplegia, septic shock, hepatopulmonary syndrome, malaria, ifosfamide neurotoxicity etc is limited but promising and commands more research. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Source: | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Methylene Blue: Revisited: J Anaesthesiol Clin Pharmacol. 2010 Oct-Dec; 26(4): 517–520. | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Ref: | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 1. Guanylate cyclase: From Wikipedia, the free encyclopedia | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 2. Methylene blue in anaphylactic shock – google search | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Perioperative beta-blockade for noncardiac surgery—proven safe or not? | ||||||||||||||||||||||||||||||||||||||||
| Don Poldermans, MD, PhD and P. J. Devereaux, MD, PhD - | ||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||
| Perioperative myocardial infarction (MI) can occur by one of two mechanisms | ||||||||||||||||||||||||||||||||||||||||
 |
||||||||||||||||||||||||||||||||||||||||
| Perioperative beta-blockade improves outcomes | ||||||||||||||||||||||||||||||||||||||||
| Don Poldermans, MD, PhD | ||||||||||||||||||||||||||||||||||||||||
| Perioperative beta-blockade improves mortality and cardiac outcomes in select high and intermediate-risk patients undergoing noncardiac surgery. | ||||||||||||||||||||||||||||||||||||||||
| Patients on chronic beta-blocker therapy should have it continued perioperatively. | ||||||||||||||||||||||||||||||||||||||||
| For patients not already on beta-blockade who are at cardiac risk, initiation of low-dose beta-blocker therapy should be considered prior to surgery; such therapy should be started approximately 1 month before surgery, with dose titration to achieve hemodynamic stability. | ||||||||||||||||||||||||||||||||||||||||
| The improved outcomes of patient with proven coronary artery disease with perioperative beta-blocker usage are emerged from the following two popular clinical trials. | ||||||||||||||||||||||||||||||||||||||||
| Perioperative Ischemic Evaluation (POISE) | Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography (DECREASE I &IV) |
| 8,351 Noncardiac surgery patients with or at risk of atherosclerotic disease | 112 underwent randomization: 59 were assigned to receive bisoprolol plus standard care and 53 to receive standard care alone |
| Extended-release metoprolol succinate started 2 to 4 hours preoperatively (100-200 mg ) and continued (200 mg/day) for 30 days. | 5-mg dose of bisoprolol was initiated 30 days prior to surgery and was titrated, if necessary, according to heart rate |
| Reduction in Cardiovascular death, nonfatal MI, or nonfatal cardiac arrest (5.8% vs 6.9% with placebo) | Death from cardiac causes or nonfatal MI was reduced from 34% in the standard-care group to 3.4% in the bisoprolol group |
| Increases in total mortality and stroke incidence(Mortality was 3.1% with metoprolol versus 2.3% with placebo) | No increase in stroke observed |
| Starting dose of metoprolol was two to eight times the commonly prescribed dose | The maintenance dose of bisoprolol was half of the maintenance dose used in POISE |
| Narrow time window for titration may be important, since the beneficial effects of beta-blockade on coronary plaque stability are likely to take weeks to develop. | Ample time for beta-blocker titration is key to stroke avoidance |
| Starting a beta-blocker at a high dose(400mg on the first day) may lead to hypotension which is a postoperative predictor of stroke |
CONCLUSIONS
| If a patient is on chronic beta-blocker therapy, do not stop it perioperatively | ||
| In a patient not on a beta-blocker, consider adding one if the patient is at intermediate or high risk of a cardiac event, but start at a low dosage (ie, 2.5 mg/day for bisoprolol and 25 mg/day for metoprolol). Treatment ideally should be started 30 days preoperatively | ||
| If a beta-blocker is not started because of insufficient time for titration, do not add one to treat tachycardia that develops during surgery, since tachycardia may represent a response to normal defense mechanisms |
Even though little doubt that perioperative beta-blockade prevents MI, looking in to the negative outcomes from POISE hypotension as the predictor of death potentially accounted for 37.3% of deaths and hypotension as the predictor of stroke accounted for 14.7% of strokes in the study.
So, in the POISE study hypotension was associated with a nearly fivefold increase in the risk of death and a doubling in the risk of stroke.
The link between hypotension and death in POISE is consistent with findings from other largest beta-blocker trials undertaken.
CONCLUSIONS
| If you want to use betablockers, use them sensibly, use them carefully, and act during surgery. If many of your patients are developing hypotension, then you are doing something wrong. | ||
| The central take-away message is that patients are unlikely to want a perioperative beta-blocker if they are unwilling to accept a probable increase in mortality or if they place three times more value on avoiding a perioperative stroke than on avoiding an MI. | ||
| It is time for perioperative medicine to enter the age of evidence-based practice and have re look in to the ACC/AHA guidelines on Perioperative Beta Blockade. |
| Evidence does not support the use of β-blocker therapy for the prevention of perioperative clinical outcomes in patients having non-cardiac surgery. The ACC/AHA guidelines committee should soften their advocacy for this intervention until conclusive evidence is available. THE LANCET |

| Assessment of LV Function – For patients with dyspnoea of unknown origin Routine perioperative evaluation of LV function is not recommended. | ||
| The 12-Lead ECG | ||
| Treadmill Exercise Stress ECG test | ||
| Dobutamine Stress Echocardiography |
| Stable angina who have significant left main coronary artery stenosis | ||
| Stable angina who have 3-vessel disease | ||
| stable angina who have 2-vessel disease with significant proximal LAD stenosis and either EF less than 0.50 or demonstrable ischemia on noninvasive testing | ||
| High-risk unstable angina or non–ST-segment elevation MI | ||
| Acute ST-elevation MI |
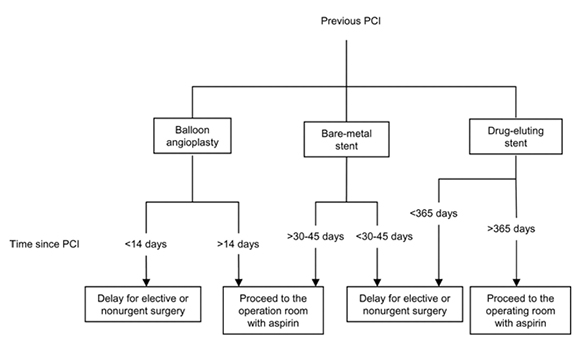
Duration of antiplatelet therapy and recommended delays for non-cardiac surgery after PCI
| Duration of antiplatelet therapy | Recommended delays for non-cardiac surgery after PCI |
| Dilatation without stenting: 2–4 weeks | Surgery postponed for 2–4 weeks (vital surgery only) |
| PCI and BMS: 4–6 weeks | Vital surgery postponed for ≥6 weeks Elective surgery postponed for ≥3 months |
| PCI and DES: 12 months | Elective surgery postponed for ≥12 months |
| Aspirin: lifelong therapy, whichever is the revascularization technique | |
Perioperative Management of Patients with Prior PCI Undergoing Noncardiac Surgery
| Surgical haemorrhagic risk | Cerebro- and cardiovascular risk | ||
| Low | Intermediate | High | |
| >6 months after MI, PCI, BMS, CABG, stroke >12 months if complications | 6–24 weeks after MI, PCI + BMS, CABG, or stroke (Ø complication); >12 months after DES; high-risk stents (long, proximal, multiple, overlapping, small vessels, bifurcation); low EF, diabetes | <6 weeks after MI, PCI, BMS, CABG; <6 months after same if complications; <12 months after high-risk DES; <2 weeks after stroke | |
| Low risk | |||
| Transfusion normally not required; peripheral, plastic, and general surgery, biopsies; minor orthopaedic, ENT, and general surgery; endoscopy; eye anterior chamber; dental extraction and surgery | Elective surgery: OK; maintain aspirin | Elective surgery: OK; maintain aspirin, clopidogrel (if prescribed) | Elective surgery: postpone; vital or emergency surgery: OK; maintain aspirin and clopidogrel |
| Intermediate risk | |||
| Transfusions frequently required; visceral surgery; cardiovascular surgery; major orthopaedic, ENT, reconstructive surgery; endoscopic urology | Elective surgery: OK; maintain aspirin | Elective surgery: postpone; surgery absolutely required: OK; maintain aspirin, clopidogrel (if prescribed) | Elective surgery: postpone; vital or emergency surgery: OK; maintain aspirin and clopidogrel |
| High risk | |||
| Possible bleeding in a closed space; intracranial neurosurgery; spinal canal surgery; eye posterior chamber surgery | Elective surgery: OK; maintain statin; withdraw aspirin (maximum 7 days) | Elective surgery: postpone; surgery absolutely required: OK; maintain aspirin, or replace aspirin by ibuprofen; stop clopidogrel | OK only for vital or emergency surgery; maintain aspirin Bridge with tirofiban/eptifibatide and heparin |
Copyright © 2013 the British Journal of Anaesthesia
Algorithm for preoperative management of patients under antiplatelet therapy
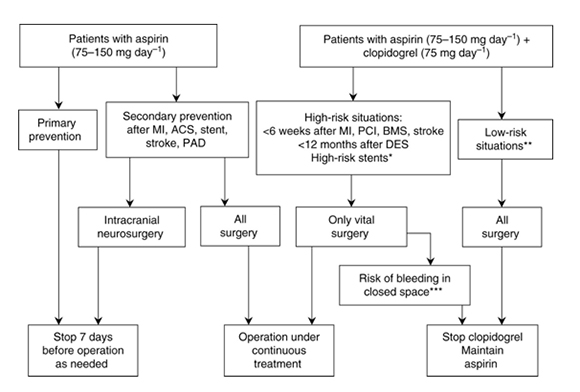
Copyright © 2013 the British Journal of Anaesthesia
| The risk/benefit ratio of preoperative withdrawal of antiplatelet drugs in order to perform a regional or neuraxial blockade is not justified |
| Informed consent for Anaesthesia |
||||||||||||||
 |
||||||||||||||
| The legal and ethical requirements related to an anaesthetist’s communication with patients in preparing them for anaesthesia, assisting them in making appropriate decisions and obtaining consent in a formal sense are complex. Doing these things well takes time, skill and sensitivity. The primary focus should be to adequately prepare patients for surgery and to ensure that they are sufficiently well informed to make the choices that best meet their own needs. | ||||||||||||||
| Anesthesiologists, should consider the need to achieve informed consent in two symbiotic senses: the legal sense and the ethical sense. | ||||||||||||||
| The best way to fulfill both senses is to be vigilant in pursuing the spirit of informed consent. Establishing the patient‐physician relationship, tailoring the disclosure of risks, and making the patient a full partner in decision making will improve the quality of the informed consent process and, as a result, decrease the likelihood of litigation. | ||||||||||||||
| Standard Disclosure Requirements for Informed Consent |
||||||||||||||
|
||||||||||||||
| Factors which anaesthetists should consider when disclosing risks to patients | ||||||||||||||
| ||||||||||||||
| Skene L, Smallwood R. Informed consent: lessons from Australia. BMJ 2002; 324:39-41 | ||||||||||||||
| Claims in negligence | ||||||||||||||
| Liability in tort would only be imposed if: | ||||||||||||||
| The anaesthetist did not disclose a material risk (breach of the duty of care – failure to inform); and | ||||||||||||||
| The risk in fact eventuated so that the patient suffered harm (injury or loss); and | ||||||||||||||
| The patient was able to persuade the court that he or she would not have agreed to the procedure if informed of the risk in question (causation). | ||||||||||||||
| You can download Anaesthesia Informed Consent as pdf or MS word format and modify according to your hospital need. | ||||||||||||||
| Downloads: | ||||||||||||||
| 1. ANESTHESIA INFORMED CONSENT 2.ANESTHESIA INFORMED CONSENT | ||||||||||||||
| Source: A Risk Management News Letter (Anaesthesia and the Law) Preferred Physicians Medical Risk Retention Group, INC | ||||||||||||||
| 2. New Texas Informed Consent Rules & Anesthesia Consent Form | ||||||||||||||
| Applications and Forms - Health Facility Program | ||||||||||||||
| Ref: | ||||||||||||||
| 1. Informed Consent Anesthesiology: October 1997 - Volume 87 - Issue 4 - p 968–978 | ||||||||||||||
| 2. Consent for Anaesthesia Revised Edition 2006 The Association of Anaesthetists of Great Britain and Ireland | ||||||||||||||
| 3. Reviews; Informed consent for anaesthesia in Australia and New Zealand The Anaesth Intensive Care 2010; 38: 809-822 | ||||||||||||||
| 4. Informed Consent for Surgical Anesthesia Care: Has the Time Come for Separate Consent? A & A February 2010 vol. 110 no. 2 280-282 | ||||||||||||||